

|
=============================================================================================== Palm Sunday Potluck Agape Meal =============================================================================================== Easter Sunrise Service April 9, 2023 @ Golden Gate Park, Hellman Hollow Picnic Area, San Francisco 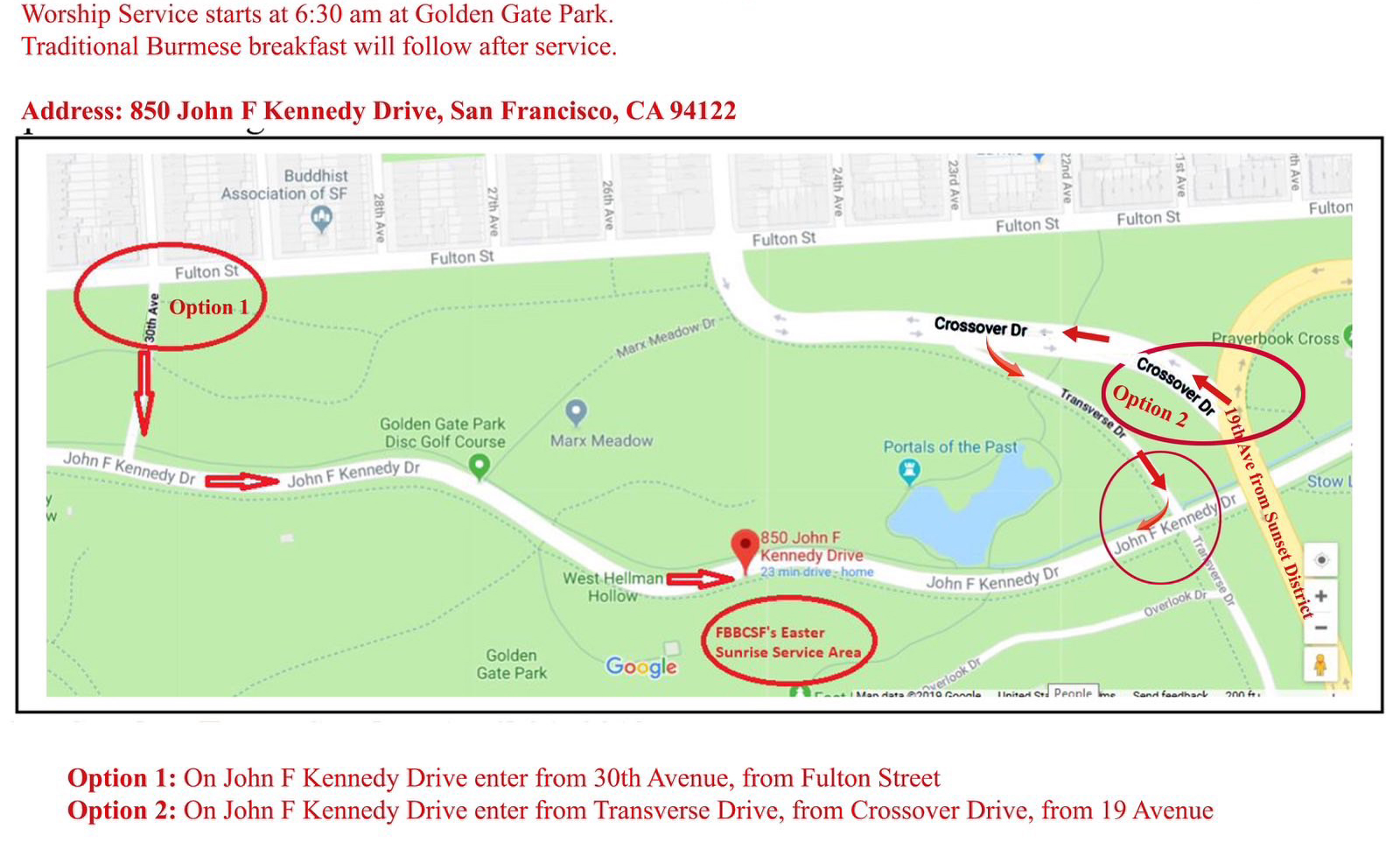 =============================================================================================== ===================================j============================================================ =============================================================================================== |